
By Sean C. Orr, M.D.
12-Minute Read
CMS Just Extended the Deadline on GENEROUS, a Drug Pricing Model That Could Reshape Your Medicaid Practice
On February 28, 2026, CMS announced it is extending the application deadline for the GENEROUS Model — one of the most consequential Medicaid drug pricing experiments in a generation. Manufacturers now have until April 30, 2026, to apply. States have until July 31.
If you’re a Florida physician who treats Medicaid patients, this isn’t background noise from Washington. This model has the potential to change your formulary access, alter your billing workflows, and redefine the economics of prescribing — particularly if you practice in oncology, rheumatology, neurology, or any specialty that relies on high-cost therapeutics.
Here’s what you need to know.
What The GENEROUS Model Actually Does
GENEROUS — which stands for GENErating cost Reductions fOr U.S. Medicaid — is a five-year voluntary pilot from the CMS Innovation Center. It runs through December 31, 2030, and the core mechanism is straightforward: CMS negotiates supplemental rebates with drug manufacturers to bring Medicaid net prices in line with what peer nations pay for the same medications.
The benchmark countries are the non-U.S. G-7 nations (the United Kingdom, France, Germany, Italy, Canada, and Japan), plus Denmark and Switzerland. The target price is based on each country’s average net price, adjusted for GDP using purchasing power parity.
In practical terms, if a drug costs Medicaid $1,000 per dose in the U.S. but averages $550 across those eight economies, GENEROUS aims to close that gap through manufacturer rebates — not by slashing your reimbursement rate, but by compelling the manufacturer to return the difference to participating states.
This is a critical distinction. Unlike the GLOBE Model (which targets Medicare Part B and directly impacts what you’re reimbursed for clinic-administered drugs), GENEROUS operates through the existing Medicaid Drug Rebate Program and layers supplemental rebates on top. Your reimbursement structure doesn’t change — the manufacturer absorbs the adjustment.
Why This Matters in Florida
Florida is one of the largest Medicaid markets in the country. The state’s managed care landscape, administered through the Agency for Health Care Administration (AHCA), already operates a Preferred Drug List that was most recently updated effective January 1, 2026. Any movement in Medicaid drug pricing at the federal level sends immediate ripples through the Florida system.
Here’s where it gets real for your practice:
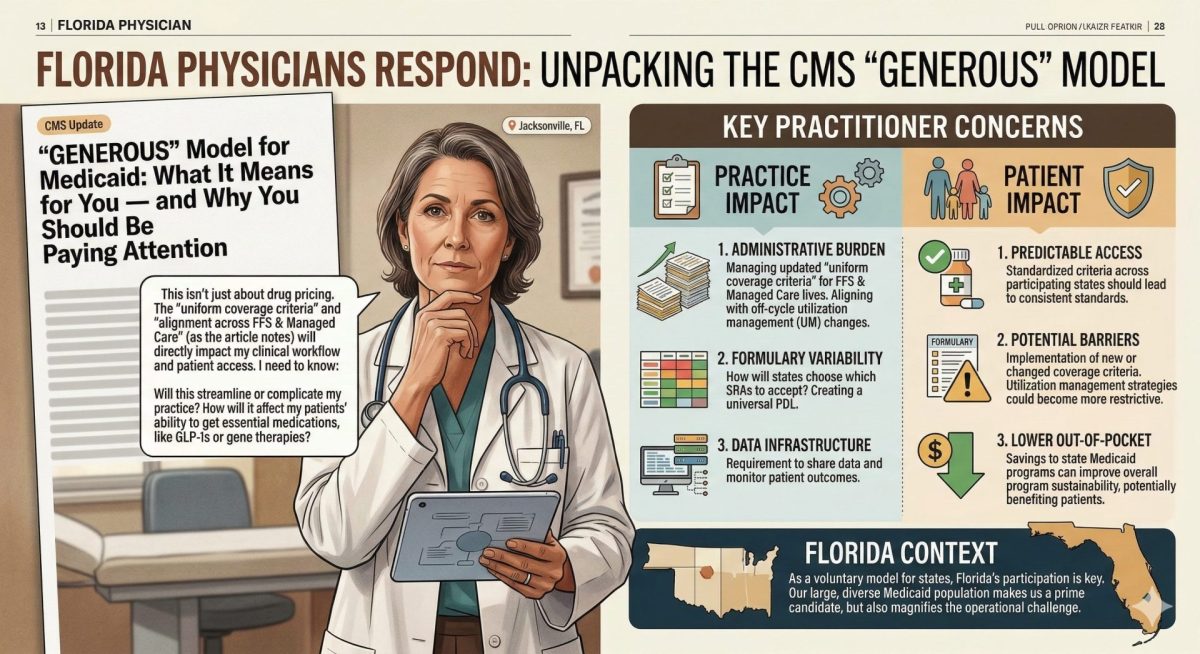
- Formulary access could improve. If manufacturers participate in GENEROUS to maintain market share in Medicaid, drugs that are currently cost-prohibitive for state programs may become accessible. That’s a direct win for your patients, and for your clinical decision-making. Fewer prior authorization battles. Fewer step-therapy workarounds. More latitude to prescribe what actually works.
- Billing complexity will increase. GENEROUS shifts documentation and rebate-validation responsibilities downstream. Whether your practice handles Medicaid billing internally or through a revenue cycle partner, expect new compliance requirements around claims processing, pricing updates, and rebate tracking. If your practice administers infused or injected medications billed through Medicaid, this is especially relevant.
- The 340B calculus doesn’t change… yet. CMS has clarified that GENEROUS supplemental rebates do not affect Medicaid “best price” calculations, which means 340B ceiling prices remain untouched. If your practice or affiliated hospital participates in the 340B program, this is important reassurance, but it’s worth monitoring as the model matures.
The Bigger Picture: GENEROUS Doesn’t Travel Alone
GENEROUS is one of three drug pricing models CMS rolled out in rapid succession. The other two — GLOBE (Global Benchmark for Efficient Drug Pricing) and GUARD (Guarding US Medicare Against Rising Drug Costs) — target Medicare Part B and Part D, respectively. Unlike GENEROUS, both GLOBE and GUARD are mandatory for manufacturers once finalized.
This is where the physician-level impact gets sharper. Under GLOBE, if the contract price of a Part B drug exceeds the international benchmark, Medicare’s reimbursement rate drops to meet it. For physicians who rely on the spread between drug acquisition cost and the ASP + 6% reimbursement to fund practice overhead, that margin could disappear entirely on certain medications.
GENEROUS, by contrast, is the gentler instrument. It’s voluntary. It targets Medicaid. And it pushes the cost adjustment upstream to manufacturers rather than downstream to providers. But make no mistake — the three models are designed to work in concert, and the direction is unmistakable: The era of the U.S. paying dramatically more than peer nations for the same medications is being actively unwound.
Does This Align With Physician Leadership?
This is the question we always ask at Florida Doctor Magazine, and the honest answer here is: it’s complicated.
The goal of lowering drug costs for Medicaid patients while preserving access to effective treatments is something every physician should support. Gross Medicaid drug spending exceeded $100 billion in 2024, a $10 billion increase from just two years earlier. Even after manufacturer rebates, net spending still topped $60 billion. Those numbers aren’t sustainable, and they translate directly into formulary restrictions, prior authorization burdens, and therapeutic limitations that compromise the care you deliver.
But physician leadership means more than endorsing good intentions. It means demanding a seat at the table where implementation decisions are made.
Here’s what concerns us:
- The model was designed without meaningful physician input. GENEROUS is structured as a negotiation between CMS and manufacturers, with states as the participating entities. Physicians are the professionals who actually prescribe these medications and manage the clinical consequences of formulary changes , and we are not at the table. That’s a structural flaw, not an oversight.
- Administrative burden flows downhill. Every pricing model that adds compliance layers eventually lands on the practice. Documentation requirements, rebate validation, pricing reconciliation… these don’t happen in a vacuum. They happen in your office, on your staff’s time, at your expense. CMS acknowledges that GENEROUS “shifts more responsibility onto providers,” but offers no corresponding investment in practice-level infrastructure to absorb it.
- Voluntary today doesn’t mean voluntary tomorrow. GENEROUS is a pilot. If it demonstrates savings, the political and regulatory incentive to make it mandatory — or to fold its mechanisms into broader Medicaid reform — is substantial. Florida physicians should engage now, while the model’s parameters are still being shaped, rather than react later when they’re fixed.
What Florida Physicians Should Do Right Now
You don’t need to wait for the state to decide whether to participate. You can act now:
- Understand your Medicaid drug exposure. Pull your prescribing data and identify which high-cost medications would likely fall within GENEROUS benchmarking. Oncology biologics, specialty injectables, and immunomodulators are the most likely targets.
- Talk to your revenue cycle team. Whether you handle billing internally or through a third party, start the conversation about what new documentation and compliance workflows GENEROUS might require.
- Engage your professional associations. The Florida Medical Association, your specialty society, and organizations like the Medical Alignment Project of The Atlas Accord should be advocating for physician representation in the state’s decision-making process around GENEROUS participation. If they’re not, push them.
- Monitor the GLOBE and GUARD rulemaking. The mandatory Medicare models are still in proposed rulemaking. The public comment period is your window to shape the final rules. Don’t let it close without your input.
- Talk to your patients. If you treat a significant Medicaid population, your patients deserve to understand that changes are coming to how their medications are priced, and that you’re engaged in making sure those changes improve their care, not just reduce a line item on a federal spreadsheet.
The Bottom Line
The GENEROUS Model represents a genuine attempt to address one of the most persistent problems in American healthcare: The fact that we pay dramatically more for prescription drugs than any comparable nation, and our most vulnerable patients — those on Medicaid — bear the consequences of that disparity through restricted formularies and limited access.
As a policy instrument, it’s thoughtfully designed. The voluntary structure, the upstream rebate mechanism, and the MFN benchmarking against peer economies all reflect lessons learned from previous failed attempts at drug pricing reform.
But thoughtful design doesn’t guarantee physician-centered implementation. That part is up to us. Florida has the Medicaid population, the clinical infrastructure, and the physician talent to be a national leader in how this model gets executed — but only if we stop treating federal policy as something that happens to us and start treating it as something we shape.
The manufacturer deadline is April 30. The state deadline is July 31. Your deadline to get informed and get involved is right now.
Florida Doctor Magazine covers the regulatory, financial, and clinical issues shaping physician practice in the Sunshine State. Subscribe to our weekly newsletter for expert-level analysis delivered free to your inbox.
floridadoctormagazine.com/subscribe
Sources
– CMS Press Release: Extending Deadline for GENEROUS Model Application. (https://www.cms.gov/newsroom/press-releases/cms-lower-drug-costs-improve-care-extending-deadline-generous-model-application)
– CMS GENEROUS Model Overview. (https://www.cms.gov/priorities/innovation/innovation-models/generous)
– HHS Press Release: New Drug Payment Model. (https://www.hhs.gov/press-room/cms-announces-new-drug-payment-model-to-better-serve-vulnerable-americans.html)
– DLA Piper: Three New Drug Pricing Models — Key Implications (https://www.dlapiper.com/en-us/insights/publications/2026/01/three-new-drug-pricing-models-for-manufacturer-rebates-key-implications)
– Paragon Health Institute: GLOBE, GUARD, and the Risk to Innovation. (https://paragoninstitute.org/paragon-prognosis/globe-guard-and-the-risk-to-innovation-examining-cms-latest-most-favored-nation-models/)
– KFF: Medicaid Enrollment & Spending Growth FY 2025–2026.(https://www.kff.org/medicaid/medicaid-enrollment-spending-growth-fy-2025-2026/)
– Florida AHCA: Medicaid Preferred Drug Program (https://ahca.myflorida.com/medicaid/prescribed-drugs/florida-medicaid-preferred-drug-program)
Frequently Asked Questions
What is the CMS GENEROUS model?
The CMS GENEROUS model is a new Medicare payment initiative designed to restructure physician reimbursement in Florida, focusing on value-based care delivery and potentially changing how primary care and specialty practices are compensated.
How does the GENEROUS model affect Florida physicians?
Florida physicians may see changes in Medicare reimbursement rates, new quality reporting requirements, and shifts in patient care delivery expectations under the GENEROUS model framework.
When does the CMS GENEROUS model take effect?
The CMS GENEROUS model is being phased in gradually, with Florida physicians expected to see initial impacts in 2026 as the program expands participation requirements.